
Multiple myeloma is personal for me. That’s because my best friend, Dr. Tom Ferguson, died from this blood cancer on April 14, 2006. Every year over 35,000 people are diagnosed with multiple myeloma and more than 12,000 die. Tom was the father of the medical self-care movement.
To quote Wikipedia, he
“…was an American medical doctor, educator, and author. He was an early advocate for patient empowerment, urging patients to educate themselves, to assume control of their own health care, and to use the Internet as a way of accomplishing those goals.”
Tom and I authored two books together and I miss him every day. One of the books was The Aspirin Handbook, (Bantam Books, 1993) and the other was a novel titled No Deadly Drug (Pocket Books, 1992). The photo at the top of this article is of Doc Tom. It sits on my computer so I can see his smile every day.
Tom got the very best treatment available at that time. Tom lived a lot longer than his doctors predicted. But like so many before him, his body ultimately surrendered to both the cancer and the aggressive treatment.
Now, though, there is a new treatment for multiple myeloma and it might have saved his life if it had been available then.
CAR-T vs. Multiple Myeloma:
The Food and Drug Administration approved a powerful new approach for the treatment of multiple myeloma in 2022. It was called ciltacabtagene autoleucel or cilta-cel for short. The treatment was sold under the brand name Carvykti. It was licensed by Janssen, a subsidiary of Johnson & Johnson and developed by Legend Biotech, a China-focused drug company that is now based in New Jersey.
This CAR-T immunotherapy was tested in both China and the US. The initial results were promising. In a trial of 97 patients, 83 percent had a complete response. These patients had all tried at least three other therapies before Carvykti. After 22 months, more than half of these individuals were still alive and their disease had not progressed. That was impressive at the time. Now, there is even better news.
The Latest Update on Carvykti Against Multiple Myeloma:
On June 3, 2025 there was an update on the Carvykti clinical trial (Journal of Clinical Oncology). The title is key:
“Long-Term (≥5-Year) Remission and Survival After Treatment With Ciltacabtagene Autoleucel in CARTITUDE-1 Patients With Relapsed/Refractory Multiple Myeloma”
As mentioned above, there were 97 multiple myeloma patients who had stopped responding to other available therapies. Many of these patients had few, if any, options left except hospice.
The investigators offered these desperate people a kind of immunotherapy called CAR-T. That abbreviation stands for Chimeric Antigen Receptor T-Cell therapy, a complicated procedure in which the patient’s white blood cells are removed and engineered to recruit T-cells against the cancer. They are then reinfused to fight the malignant cells.
Until now, CAR-T approaches have mostly been developed for other blood cancers, such as leukemia or lymphoma. The new therapy worked surprisingly well for multiple myeloma.
One-third of the patients who got the therapy five years ago are still cancer-free. The researchers note:
“To our knowledge, our data provide the first evidence that cilta-cel is potentially curative in patients with RRMM.” [RRMM stands for relapsed or refractory multiple myeloma.]
Oncologists are excited about the unprecedented results reported in the Journal of Clinical Oncology, June 3, 2025).
Dr. Norman Sharpless told the New York Times (June 3, 2025):
“’In my 30 years in oncology, we haven’t talked about curing myeloma,’ said Dr. Norman Sharpless, a former director of the National Cancer Institute who is now a professor of cancer policy and innovation at the University of North Carolina School of Medicine. ‘This is the first time we are really talking seriously about cure in one of the worst malignancies imaginable.’
“And for those like the patients in the new study who are living at least five years — so far — without disease, the outcome ‘really is eye-popping,’ Dr. Sharpless said.”
“’That’s getting to a point where you wonder if it will ever come back,’ he added.”
If My Friend Tom Had Received Carvykti…
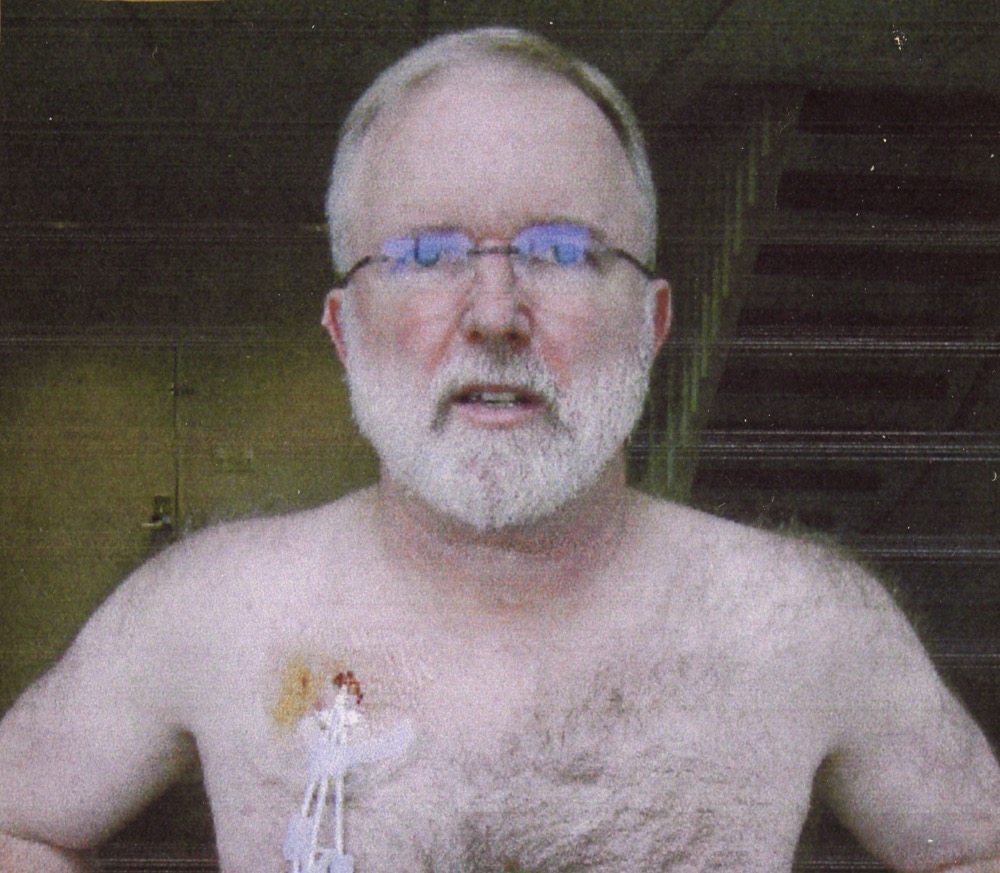
When Tom’s cancer returned, he had a bone marrow transplant. I remember trying to protect him from infection because his immune system had been decimated by heavy-duty chemotherapy. The photo below is Tom at the University of Arkansas Medical Center where he had recently undergone his bone marrow transplant. You can see the ports that were implanted. He recovered and did well for quite a while. Tom lived a lot longer than most multiple myeloma patients at that time. Carvykti might have changed the outcome.
The Downsides of CAR-T for Multiple Myeloma:
There are several challenges with treatments like CAR-T. In many cases, insurance companies and guideline committees reserve these approaches as a last resort. That’s partly because they come with serious side effects. Carvykti can trigger fever, infections, fatigue, headache, diarrhea, muscle pain, nausea, low blood pressure and neurological symptoms. There is also the price tag! More about that momentarily.
What if Carvykti was tried earlier in the treatment process?
The New York Times offers this professional perspective:
“Dr. Kenneth Anderson, a myeloma expert at Dana-Farber Cancer Institute who was not involved with the study, said that if the treatment is used as a first-line treatment, ‘cure is now our realistic expectation.’”
In addition to adverse reactions, the biggest drawback of this CAR-T treatment is the price tag. According to the NYT, the list price for Carvykti is over $555,000. But that may not include many additional costs including post-treatment expenses. Some estimate that the total cost of CART-T treatments could exceed $1 million if patients experience serious adverse reactions that require hospitalizations.
Many insurance companies balk at paying over half a million dollars for this kind of treatment, unless all other options have been exhausted. There may also be a co-pay depending upon coverage.
What this means is that many patients will be on death’s doorstep before they can get access. As mentioned, some investigators hope that if the treatment were administered earlier in the disease, it might prove to be a cure for more patients.
Carvykti Is an Orphan Drug:
Like many of the newest cancer drugs, Carvykti has received Orphan Drug Designation from the FDA. When this category was first established, it was for “significant drugs of limited commercial value.”
The expectation was that pharmaceutical companies would not charge excessively for medicines that would be taken by relatively few people. Few, of course, is a relative term. It could be thousands of cancer patients. Congress gave drug companies incentives to develop orphan drugs on the grounds that they probably would not break even or make much money.
Drug companies quickly saw an opportunity, though. Orphan drugs are now huge money makers for the pharmaceutical industry. Some treatments for rare genetic conditions can cost millions. Many of the latest cancer treatments are also incredibly expensive. How many people will be able to afford extraordinary advances from breakthroughs like Carvykti?
Please do not get me started on the high cost of cancer drugs! Should you wish to read my thoughts on this topic, here is a link.
To Learn More:
If you would like to learn more about cancer therapy you might want to listen to our radio show/podcast: Show 1029: How to Mobilize the Immune System to Fight Cancer.
We would also like to read your story. If you have been treated for cancer, please let us know how it went. If you think this article is important, please share it with friends and family. You can do so easily by scrolling to the top of the post and clicking on the icons for email or social media. If you appreciate our articles, please encourage acquaintances to sign up for our free newsletter at this link. Thank you for supporting our work.
Citations
- Jagannath, S., et al, "Long-Term (≥5-Year) Remission and Survival After Treatment With Ciltacabtagene Autoleucel in CARTITUDE-1 Patients With Relapsed/Refractory Multiple Myeloma," Journal of Clinical Oncology, June 3, 2025, doi: 10.1200/JCO-25-00760

 treatment for multiple myeloma looks like a game changer. But a price of over $500,000 is scary!&message=Multiple Myeloma Meets Its Match with CAR-T – Can Cancer Patients Afford It?&redirect_asPath=https://www.peoplespharmacy.com/articles/does-car-t-offer-hope-for-multiple-myeloma-cancer){kind=link}